You’ve noticed the hair at your crown getting thinner. Maybe it started years ago with a small patch you could cover, but now the area’s wider, shinier, and the hair won’t grow back no matter what you try. When you part your hair, you see smooth scalp where follicles used to be. That’s not typical hair loss. That’s scarring.
Central centrifugal cicatricial alopecia, or CCCA, is the most common form of permanent hair loss in women of African descent. It starts at the vertex (the crown) and spreads outward in a circular pattern, destroying hair follicles as it goes. Once a follicle scars over, it’s gone. The hair that grew there won’t come back. But here’s what matters: if you catch it early, you can stop it from spreading further.
This isn’t about vanity. CCCA affects up to 17% of Black women in some studies, yet it remains underdiagnosed and undertreated in mainstream dermatology. Many women lose years of potential intervention because they’re told it’s ‘just stress’ or ‘normal aging.’ It’s neither. CCCA is a chronic inflammatory condition that requires medical treatment, and the earlier you start, the more hair you can save.
What CCCA Actually Is and How It Differs from Other Hair Loss
CCCA belongs to a category called primary cicatricial alopecias (scarring hair loss). Unlike androgenetic alopecia (pattern baldness) or telogen effluvium (stress shedding), where follicles shrink but remain intact, CCCA involves permanent destruction of the follicle itself. Inflammation targets the upper portion of the hair follicle, specifically the bulge region where stem cells live. When that area scars, the follicle can’t regenerate.
The ‘central centrifugal’ part describes the pattern: it begins at the center of the scalp (the vertex or crown) and spreads outward in expanding circles. Early on, you might notice tenderness, itching, or burning at the crown. Some women report a painful scalp before visible hair loss appears. Others see thinning first, then realize the follicles underneath have scarred.
What makes CCCA distinct is that the scarring happens from the inside out. The surface of your scalp might look relatively normal for a while, but underneath, follicles are being replaced by fibrous tissue. By the time you see a smooth, shiny patch with no visible pores, the damage is advanced. That’s why dermatologists emphasize early detection, ideally when symptoms start but before widespread scarring occurs.
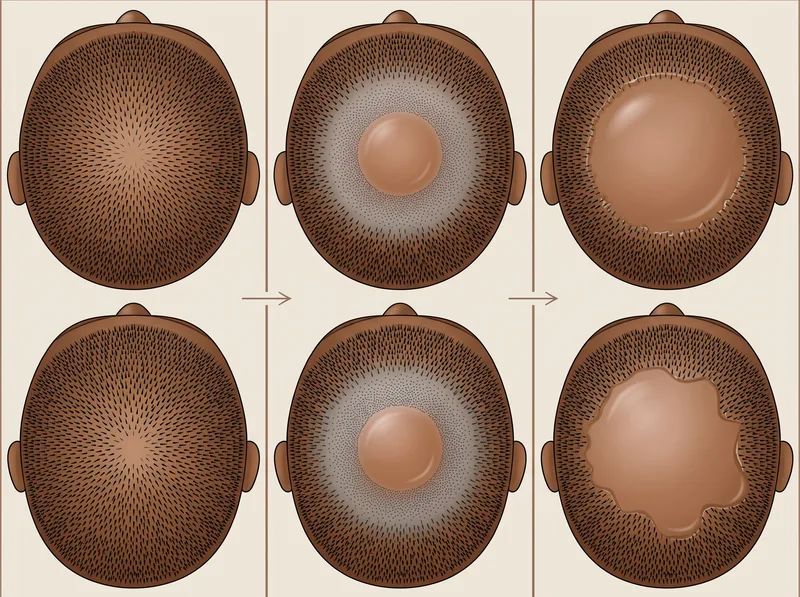 CCCA typically progresses in stages, starting with subtle thinning at the crown and expanding outward over months to years
CCCA typically progresses in stages, starting with subtle thinning at the crown and expanding outward over months to years
What Causes CCCA and Why It Affects Black Women Disproportionately
The exact cause of CCCA isn’t fully understood, but research points to a combination of genetic susceptibility and environmental triggers. It’s not a single-factor disease. You can’t get CCCA from one bad relaxer or one tight hairstyle. But if you’re genetically predisposed, repeated trauma and chronic inflammation can trigger the scarring process.
Genetic factors are significant. Studies have identified mutations in the PAD13 gene, which codes for a protein involved in hair shaft formation, in some women with CCCA. This suggests an inherited vulnerability in follicle structure. If your mother, grandmother, or sisters have central scalp thinning, your risk is higher. But genetics alone don’t explain the full picture.
Traction and chemical damage act as triggers in susceptible individuals. Decades of tight braiding, weaves with tension at the crown, chemical relaxers, and high-heat styling can create chronic low-grade inflammation. The crown is particularly vulnerable because it bears the most tension in many protective styles and experiences the highest heat exposure during flat ironing. Over time, this repetitive trauma may activate the inflammatory cascade in genetically predisposed follicles.
It’s critical to understand this isn’t about blaming hairstyles. Many Black women use these practices without developing CCCA. The condition occurs when genetic susceptibility meets environmental stress. Cultural context matters here: for decades, Black women faced workplace discrimination that pressured them toward chemically straightened or tightly pulled-back hair. CCCA’s prevalence reflects systemic issues, not personal failure.
Emerging research also suggests sebum composition differences and bacterial colonization patterns may play roles. Some studies have found altered lipid profiles in CCCA-affected scalps and changes in the scalp microbiome. This is an active area of investigation, with implications for future treatments targeting inflammation at its source.
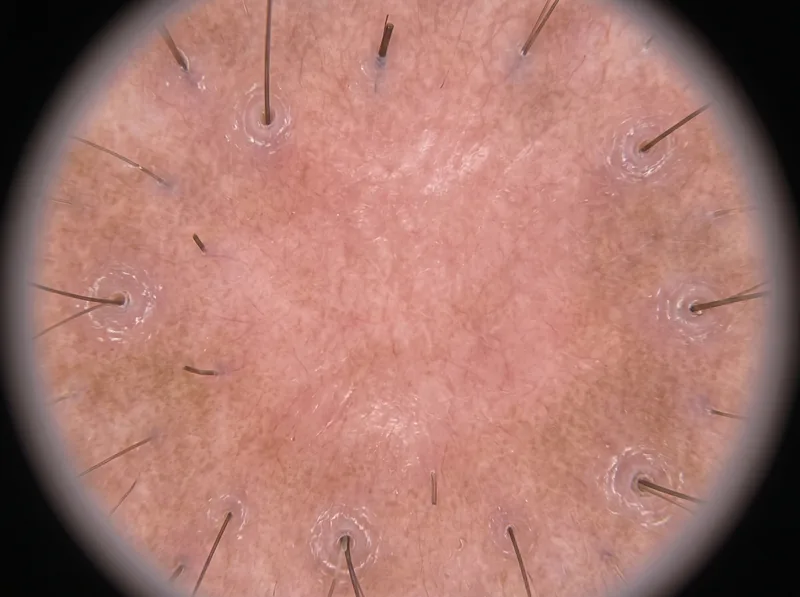 Dermoscopy reveals diagnostic features of CCCA including absence of follicular openings in affected areas and perifollicular inflammation at the margins
Dermoscopy reveals diagnostic features of CCCA including absence of follicular openings in affected areas and perifollicular inflammation at the margins
Recognizing the Symptoms and Getting a Proper Diagnosis
Early CCCA can be subtle. You might notice your part getting wider at the crown, or feel tenderness when you touch that area. Some women describe a burning or stinging sensation, especially after styling. Others see small bumps (follicular papules) or notice their hair breaking more easily at the crown than elsewhere. If you’re experiencing any of these, don’t wait.
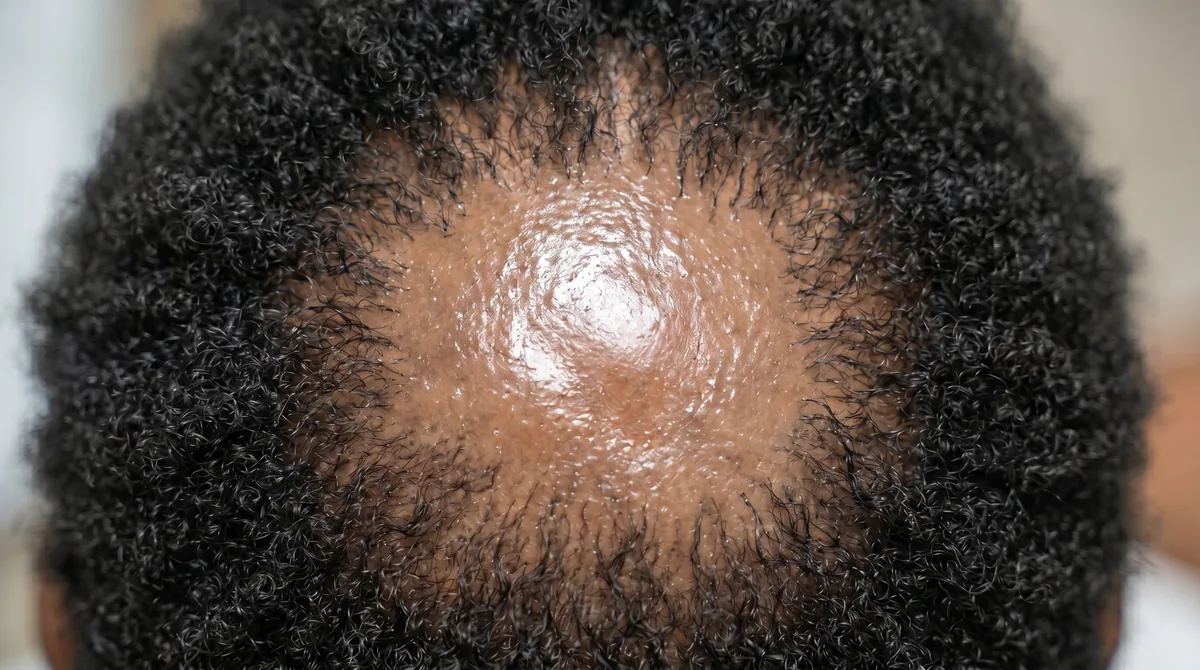
As CCCA progresses, the central bald patch becomes more obvious. The affected scalp looks smooth and shiny because the follicles are gone. If you look closely, you won’t see the tiny dots (follicular ostia) that mark healthy pores. The border between affected and unaffected areas is usually distinct, and the hair loss spreads symmetrically outward. In advanced cases, the scarred area can extend several centimeters from the crown, sometimes reaching the frontal hairline.
Diagnosis requires a dermatologist, ideally one experienced with hair disorders. They’ll perform a clinical examination, looking at the pattern and checking for follicular dropout. Dermoscopy (trichoscopy) is essential. Under magnification, CCCA shows absent follicular openings in scarred areas, perifollicular scaling at the margins, and sometimes pinpoint white dots (fibrotic scarring). In active disease, you’ll see signs of inflammation.
A scalp biopsy is the gold standard for confirming CCCA. A 4mm punch biopsy taken from the active border (not the center of the scar) will show characteristic features: premature desquamation of the inner root sheath, follicular dropout, perifollicular fibrosis, and lymphocytic inflammation around the upper follicle. The biopsy also rules out other scarring alopecias like lichen planopilaris or frontal fibrosing alopecia, which require different treatments.
Don’t self-diagnose. Other conditions can mimic CCCA, including tinea capitis (scalp fungus), discoid lupus, and even severe seborrheic dermatitis. Getting the right diagnosis early means you can start treatment before more follicles are lost permanently.
Medical Treatments That Can Stop Progression
There’s no cure for CCCA, but medical treatment can halt or significantly slow the inflammatory process, preventing further scarring. The goal is to preserve the follicles you still have. Once scarring is established, those follicles won’t regenerate, but you can stop the condition from spreading.
Topical corticosteroids are the first-line treatment. High-potency steroids like clobetasol propionate 0.05% solution or foam are applied directly to the affected area to suppress inflammation. These are typically used daily or every other day for several months. Intralesional corticosteroid injections (triamcinolone acetonide) are also effective, particularly for active, symptomatic areas. A dermatologist injects small amounts directly into the scalp at the border of the scarring. This delivers anti-inflammatory medication exactly where it’s needed.
Oral medications may be necessary for more aggressive disease. Low-dose doxycycline (50-100mg daily) has anti-inflammatory properties beyond its antibiotic effects and is commonly prescribed for CCCA. Some dermatologists use hydroxychloroquine (Plaquenil), an antimalarial drug with immunomodulatory effects, particularly when there’s significant inflammation. Oral corticosteroids (prednisone) are reserved for acute flares but aren’t sustainable long-term due to side effects.
Topical minoxidil (5%) can be added to stimulate any remaining follicles and improve hair density in the surrounding areas, though it won’t reverse scarring. Some dermatologists prescribe topical antibiotics (clindamycin solution) to address bacterial colonization that may worsen inflammation. Combination therapy (steroids plus antibiotics plus minoxidil) is common and often more effective than monotherapy.
Newer treatments under investigation include JAK inhibitors (tofacitinib, ruxolitinib), which target specific inflammatory pathways, and platelet-rich plasma (PRP) injections to promote healing and stimulate remaining follicles. These aren’t yet standard of care for CCCA but show promise in early studies. Treatment requires patience. It can take 6-12 months to see stabilization, and you’ll need ongoing maintenance therapy to prevent relapse.
 Reducing tension and heat exposure while maintaining scalp health can slow CCCA progression, though these changes alone cannot reverse established scarring
Reducing tension and heat exposure while maintaining scalp health can slow CCCA progression, though these changes alone cannot reverse established scarring
Hair Care Modifications That Support Treatment
Medical treatment is essential, but hair care changes can support healing and reduce ongoing trauma. This isn’t about abandoning your cultural hairstyles. It’s about reducing tension, heat, and chemical exposure while your scalp heals. Many women successfully manage CCCA while maintaining their hair identity.
Eliminate or drastically reduce tension. Tight braids, cornrows, weaves sewn onto tight braids, high ponytails, and buns that pull at the crown all create traction. If you wear protective styles, ask your stylist to braid loosely, especially at the crown and edges. Take breaks between installations. Consider styles that distribute tension more evenly or don’t require tension at all, like twist-outs, braid-outs, or loose, chunky twists.
Minimize heat styling. High-heat flat irons (above 350°F) can damage already vulnerable follicles. If you straighten your hair, use the lowest effective temperature, apply heat protectant, and limit frequency. Air-drying or low-heat diffusing is gentler. Some women transition to heat-free styling methods during active treatment, then reintroduce heat cautiously once the condition stabilizes.
Reconsider chemical relaxers. The combination of sodium hydroxide (lye) or calcium hydroxide (no-lye) relaxers and CCCA is controversial. While relaxers alone don’t cause CCCA, they can exacerbate inflammation in susceptible scalps. Many dermatologists recommend discontinuing relaxers during active disease. If you choose to relax, stretch the time between applications, avoid overlapping, and consider switching to less aggressive formulations or texturizers.
Scalp health becomes paramount. Keep your scalp clean but not stripped. Shampoo regularly (weekly or more often if needed) to remove buildup and reduce bacterial colonization. In the Gulf region, where mineral-heavy water is common, a chelating shampoo can prevent mineral deposits that worsen inflammation. Regrowth+ chelating shampoo, for example, removes calcium and magnesium buildup without harsh sulfates, which is particularly helpful for women managing both CCCA and hard water effects.
Moisturize and protect. CCCA-affected scalps often have altered sebum production. Use lightweight, non-comedogenic oils (jojoba, argan) or water-based leave-ins to keep the scalp hydrated without clogging follicles. Avoid heavy petroleum-based products that can trap heat and bacteria. At night, protect your hair with a satin or silk bonnet or pillowcase to reduce friction.
Long-Term Management and What to Expect
CCCA is a chronic condition. Even with successful treatment, you’ll need ongoing management to prevent relapse. Think of it like managing a chronic skin condition such as eczema or psoriasis. Flares can happen, especially during times of stress, illness, or if you return to high-risk hair practices. The goal is long-term control, not a one-time fix.
Most women see stabilization within 6-12 months of starting treatment. Symptoms like pain, itching, and burning typically improve first, followed by a halt in hair loss progression. You might see some regrowth at the margins where follicles weren’t completely scarred, but don’t expect full restoration in areas with established scarring. The scarred center won’t regrow hair without surgical intervention.
Maintenance therapy is essential. Many dermatologists recommend continuing topical treatments (often at reduced frequency) indefinitely. You might step down from daily clobetasol to twice-weekly application, or continue oral doxycycline at a low dose long-term. Regular follow-ups (every 3-6 months) allow your dermatologist to monitor for disease activity and adjust treatment as needed.
Hair transplantation is an option for stable, well-controlled CCCA, but only after the inflammatory process has been quiet for at least 12-18 months. Transplanting into active inflammation will fail. Follicular unit extraction (FUE) is preferred over strip harvesting because it creates less tension. Not all surgeons are experienced with CCCA, so seek a specialist who understands scarring alopecias and has worked with textured hair.
Psychological support matters. Permanent hair loss affects identity, self-esteem, and mental health. Many women with CCCA experience depression, anxiety, and social withdrawal. Support groups (online and in-person), therapy, and connecting with others who understand the condition can be invaluable. Organizations like the Cicatricial Alopecia Research Foundation (CARF) provide resources and community.
For some women, wigs, toppers, or creative styling become part of their solution. There’s no shame in choosing these options. The goal is to feel confident and comfortable while managing a chronic medical condition. What matters is that you have access to accurate information, effective treatment, and support to make choices that work for your life.
References
- Central Centrifugal Cicatricial Alopecia: Challenges and Solutions - American Academy of Dermatology
- Genetic Risk Factors for Central Centrifugal Cicatricial Alopecia in African Americans - PubMed
- Pathogenesis and Management of Central Centrifugal Cicatricial Alopecia - PubMed Central
- Treatment Guidelines for Primary Cicatricial Alopecias - Journal of the American Academy of Dermatology