This article contains affiliate links. See our affiliate disclosure for details.
You’ve been using minoxidil for three months. Maybe four. The bottle says you should see results by now, but when you look in the mirror, you’re not sure anything’s changed. Or worse, your hair looks thinner than when you started.
Here’s what nobody tells you: minoxidil works. The science is solid. But if you’re in the Gulf region, there’s a critical factor that can sabotage your results before the treatment even reaches your follicles. It’s not genetics. It’s not the product quality. It’s your water.
This is the complete guide to using minoxidil for hair loss in the Gulf, covering everything from how the molecule actually works to why environmental factors here create unique challenges. We’ll also address the hard truth about timelines, side effects, and what to do when results plateau. By the end, you’ll know exactly how to maximize your treatment and avoid the mistakes that cause most people to quit too early.
What Is Minoxidil and How Does It Actually Work?
Minoxidil is a vasodilator that was originally developed to treat high blood pressure. In the 1980s, researchers noticed that patients taking oral minoxidil were experiencing unexpected hair growth as a side effect. That observation led to the development of topical minoxidil (brand name Rogaine), which became the first FDA-approved treatment for pattern hair loss.
At the molecular level, minoxidil works through several mechanisms. It opens potassium channels in the cells surrounding hair follicles, which triggers a cascade of effects: increased blood flow to the follicle, prolonged anagen (growth) phase, and stimulation of vascular endothelial growth factor (VEGF), which promotes new blood vessel formation around follicles.
The result? Follicles that were shrinking and producing thinner hair can reverse course. Miniaturized hairs become thicker. Dormant follicles can reactivate. But here’s the catch: minoxidil doesn’t work on completely dead follicles. If the follicle has been dormant for more than five years, the chances of revival drop significantly.
There are two main concentrations available: minoxidil 2% and minoxidil 5%. Studies show that 5% minoxidil is significantly more effective than 2%, with approximately 45% of users experiencing moderate to dense regrowth at 48 weeks, compared to 30% with the 2% formulation. The 5% version is now approved for both men and women in most countries, though women were initially limited to 2% due to concerns about facial hair growth.
Minoxidil comes in two forms: liquid solution and foam. The foam formulation was developed to address irritation issues caused by propylene glycol, a carrier ingredient in the liquid version. Both are equally effective, but foam tends to cause less scalp irritation and dries faster, making it more convenient for daytime use.
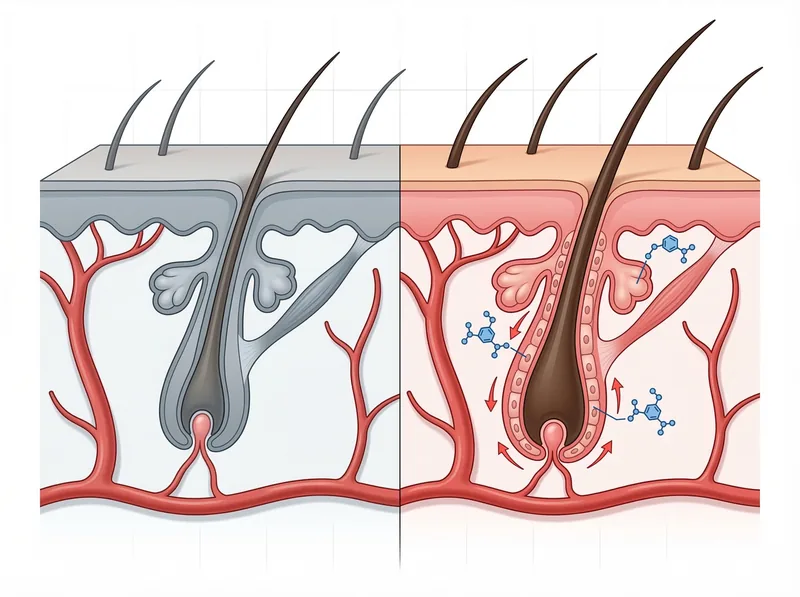 How minoxidil works: The molecule opens potassium channels in follicle cells, extending the growth phase and increasing blood flow to the scalp.
How minoxidil works: The molecule opens potassium channels in follicle cells, extending the growth phase and increasing blood flow to the scalp.
Who Should Use Minoxidil (and Who Shouldn’t)
Minoxidil is FDA-approved for androgenetic alopecia (pattern hair loss) in both men and women. This is the most common type of hair loss, affecting roughly 50% of men by age 50 and 40% of women by menopause. If you’re experiencing gradual thinning at the crown or temples (men) or diffuse thinning across the top of the scalp (women), minoxidil is a scientifically validated option.
It’s also used off-label for other conditions. Some dermatologists prescribe it for alopecia areata (patchy hair loss), telogen effluvium (stress-related shedding), and even beard growth, though the evidence for these uses is less strong. The American Academy of Dermatology notes that minoxidil can help with various forms of hair loss, but results vary significantly depending on the underlying cause.
You should NOT use minoxidil if you have an undiagnosed scalp condition (especially if there’s redness, scaling, or infection), if you’re pregnant or breastfeeding, or if you have a history of heart problems without consulting a cardiologist first. While topical minoxidil has minimal systemic absorption, there have been rare reports of cardiovascular effects in people with pre-existing conditions.
Age matters too. Minoxidil works best when started early, ideally within the first five years of noticing hair loss. The longer follicles remain dormant, the harder they are to revive. If you’re in your 20s or 30s and just starting to see thinning, you’re in the ideal window. If you’re 50+ and have been bald for a decade, manage your expectations, you may see some improvement, but dramatic regrowth is unlikely.
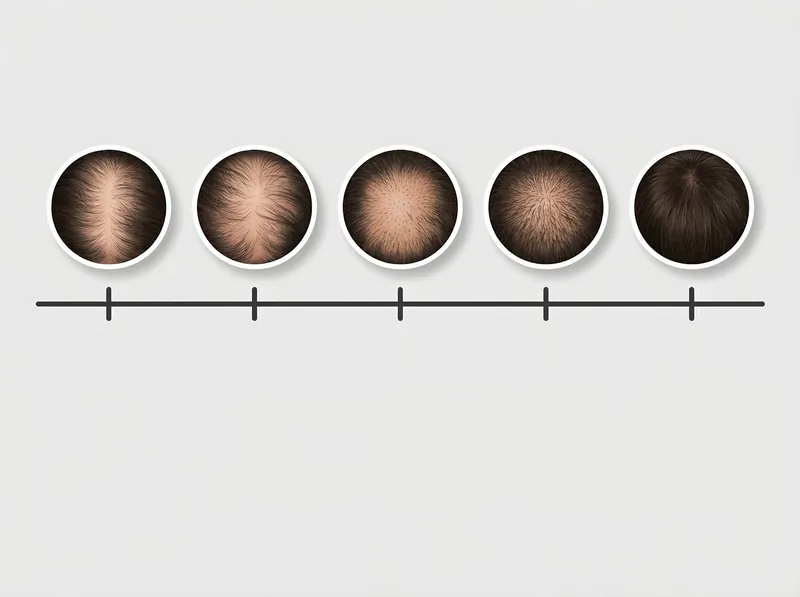 Minoxidil results follow a predictable timeline, with initial shedding in weeks 2-8, followed by visible regrowth starting around month 4.
Minoxidil results follow a predictable timeline, with initial shedding in weeks 2-8, followed by visible regrowth starting around month 4.
How to Use Minoxidil: Application, Dosage, and Timing
The standard protocol is simple: apply 1ml of minoxidil solution (or half a capful of foam) to the affected area twice daily, roughly 12 hours apart. Morning and night. Every day. Consistency is everything. Missing doses doesn’t just slow progress, it can cause you to lose ground.
Here’s how to apply it correctly. Start with a completely dry scalp. If you’ve just washed your hair, wait at least 2-3 hours before applying minoxidil (or apply it before showering and wait 4 hours before washing). Part your hair to expose the scalp in the thinning area. For foam, dispense the product into your hands and massage it directly into the scalp, not the hair. For liquid, use the dropper to apply directly to the scalp, then spread with your fingertips.
Do NOT apply more than the recommended dose. More isn’t better. Your scalp can only absorb so much, and excess product just runs off or increases the risk of side effects. The 1ml dose has been clinically improved for maximum absorption.
Timing your application matters more than you think. Apply minoxidil to a clean scalp whenever possible. If you use other topical treatments (like tretinoin or corticosteroids), apply minoxidil first and wait at least 30 minutes before applying anything else. This prevents dilution and ensures maximum absorption.
One critical detail: don’t wash your hair immediately after application. Minoxidil needs at least 4 hours to fully absorb. If you shower within that window, you’re literally washing away the treatment. This is why many people prefer applying it at night and washing their hair in the morning, or applying it in the morning and showering at night.
Can you use minoxidil once daily instead of twice? Research suggests that once-daily application of 5% minoxidil can be effective, though results are generally better with twice-daily use. If you’re going to do once daily, use the 5% concentration and apply it at night when absorption time is longer.
The Minoxidil Timeline: What to Expect Month by Month
Let’s be brutally honest about timelines. You will NOT see results in week two. Or week four. In fact, your hair will probably look worse before it looks better. This is normal. It’s called the minoxidil shed, and it’s actually a sign the treatment is working.
Here’s what typically happens. Weeks 1-2: Nothing visible. You’re establishing the routine. Weeks 2-8: The shedding phase begins. You’ll notice increased hair fall in the shower, on your pillow, when you run your hands through your hair. This happens because minoxidil is pushing dormant follicles into the growth phase, which means the old, weak hairs fall out to make room for new growth. It’s unsettling, but it’s temporary.
Months 3-4: Shedding slows. You might start seeing fine, baby hairs (vellus hairs) along the hairline or in thinning areas. These are new hairs in the early growth stage. They’ll look wispy and light-colored at first. Months 4-6: The new hairs start to thicken and darken. This is when most people notice the first real improvement in density. Photos from month 0 and month 6 should show a visible difference.
Months 6-12: Continued improvement. Hair becomes thicker, longer, and more pigmented. By month 12, you’ve reached your peak results with minoxidil alone. After that, the goal is maintenance. Some people continue to see gradual improvement up to 18 months, but the most dramatic changes happen in the first year.
If you’re not seeing ANY improvement by month 6, something’s wrong. Either the diagnosis is incorrect (it’s not androgenetic alopecia), the follicles are too far gone, or there’s an absorption issue. This is where environmental factors come into play, which we’ll address in the next section.
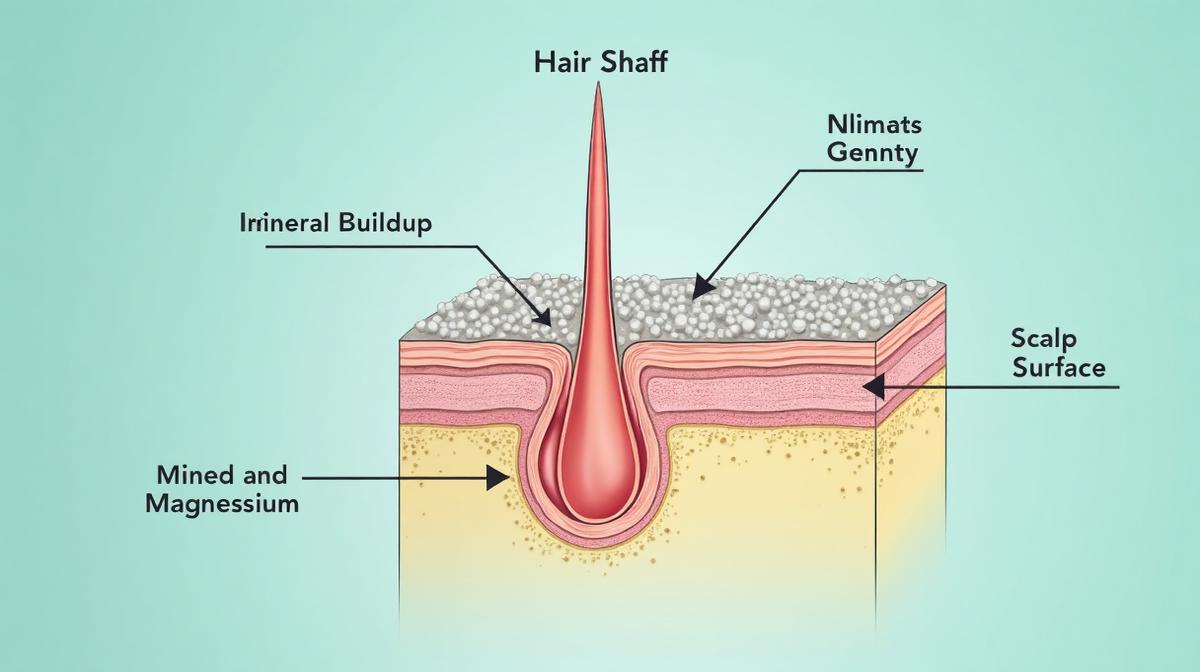
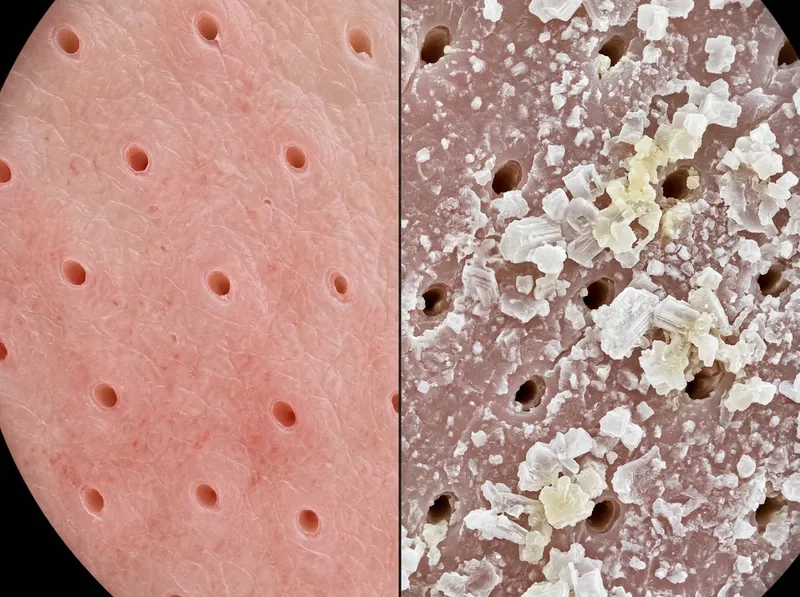 Hard water minerals create a barrier on the scalp that can prevent minoxidil from reaching hair follicles effectively.
Hard water minerals create a barrier on the scalp that can prevent minoxidil from reaching hair follicles effectively.
Why Hard Water in the Gulf Sabotages Minoxidil Results
Here’s the factor that almost no one discusses: hard water can significantly reduce minoxidil’s effectiveness. And if you’re living in the Gulf region, you’re dealing with some of the hardest water in the world.
Hard water contains high concentrations of dissolved minerals, primarily calcium and magnesium. In the Gulf, total dissolved solids (TDS) levels regularly exceed 400-600 ppm, compared to 50-150 ppm in regions with naturally soft water. When you wash your hair with this water, those minerals don’t just rinse away, they bond to your hair and scalp, creating a coating that acts as a physical barrier.
This barrier has two effects on minoxidil. First, it prevents the active ingredient from penetrating the scalp effectively. Minoxidil needs direct contact with the follicle cells to work, but if there’s a layer of mineral buildup in the way, absorption drops. Second, the minerals alter the pH of your scalp, creating an environment that can reduce minoxidil’s stability and effectiveness.
You can see this buildup yourself. If your scalp feels rough or gritty to the touch, if you have persistent flaking that isn’t dandruff, or if your hair feels coated and dull even after washing, you’re dealing with mineral deposits. This is especially common if you’re using desalinated water, which is standard in many Gulf cities, the desalination process removes salt but often leaves calcium and magnesium behind.
The solution isn’t to stop washing your hair (that creates its own problems). The solution is to use a chelating shampoo before applying minoxidil. Chelating agents bind to mineral ions and allow them to be rinsed away, restoring a clean surface for treatment absorption. A chelating shampoo like Regrowth+ is specifically formulated to remove hard water buildup without stripping your scalp’s natural oils, which is critical when you’re using an active treatment like minoxidil.
The protocol: wash with a chelating shampoo 2-3 times per week, especially before applying minoxidil. On non-chelating days, use a gentle, sulfate-free shampoo. This keeps your scalp clean and receptive without over-stripping. It’s a simple adjustment that can make the difference between mediocre results and visible regrowth. For more detail on how hard water affects hair health in the region, see our guide on hard water in the GCC.
Common Side Effects and How to Manage Them
Most people tolerate minoxidil well, but side effects do happen. The most common is scalp irritation, redness, itching, dryness, or flaking. This is usually caused by propylene glycol in the liquid formulation, not the minoxidil itself. If you experience this, switch to the foam version, which is propylene glycol-free. About 70% of people who react to the liquid can use the foam without issues.
Unwanted facial hair growth is another concern, particularly for women. This happens when minoxidil drips down from the scalp onto the forehead or face during application. The solution is careful application (use the dropper precisely or apply foam with clean hands) and washing your face after applying the treatment. If facial hair does develop, it typically reverses within a few months of stopping minoxidil.
Some users report increased heart rate or dizziness, especially when first starting treatment. This is rare with topical use (systemic absorption is minimal), but if it happens, stop using the product and consult a doctor. Do NOT ignore cardiovascular symptoms, even if they seem mild.
The most psychologically difficult side effect is the initial shedding phase. We covered this in the timeline section, but it’s worth repeating: increased shedding in weeks 2-8 is normal and expected. It does NOT mean the treatment is making your hair loss worse. It’s the old, weak hairs making way for new growth. Push through it. Most people who quit minoxidil do so during this phase, which means they never get to see the results they were working toward.
If you experience severe or persistent side effects, scalp pain, swelling, rapid heartbeat, unexplained weight gain, or facial swelling, stop using minoxidil immediately and see a healthcare provider. These are signs of a serious reaction or systemic absorption issue.
Minoxidil for Women: What’s Different?
Women can absolutely use minoxidil, and it’s one of the few hair loss treatments with solid evidence in female pattern hair loss. But there are some important differences in how women experience and use the treatment.
First, the pattern of hair loss is different. Men typically lose hair at the temples and crown in a predictable pattern (the Norwood scale). Women usually experience diffuse thinning across the top of the scalp, with the hairline remaining intact (the Ludwig scale). This means women often need to apply minoxidil over a larger area.
Second, women were historically limited to minoxidil 2% due to concerns about unwanted facial hair growth with the 5% formula. However, more recent studies show that 5% minoxidil is safe and significantly more effective for women, with only a small increase in facial hair risk. Many dermatologists now prescribe 5% for women, especially those who don’t respond adequately to 2%.
Third, women are more likely to experience shedding during the initial phase, possibly because female hair loss often involves a larger number of follicles in the telogen (resting) phase. This makes the first 2-3 months particularly challenging psychologically. Support from a dermatologist or trichologist during this phase can be invaluable.
Pregnancy and breastfeeding are absolute contraindications. Minoxidil is classified as Category C for pregnancy (animal studies show risk, but human data is limited). If you’re trying to conceive, pregnant, or nursing, do NOT use minoxidil. Discuss alternative treatments with your doctor.
For women dealing with hormonal hair loss (related to PCOS, thyroid issues, or menopause), minoxidil can be effective, but it works best as part of a complete treatment plan that addresses the underlying hormonal imbalance. Minoxidil treats the symptom (hair loss), not the cause (hormone changeion).
Combining Minoxidil with Other Treatments
Minoxidil works well, but it works even better when combined with other evidence-based treatments. The most common combination is minoxidil + finasteride (for men) or minoxidil + spironolactone (for women). These medications address different aspects of hair loss: minoxidil stimulates growth, while finasteride/spironolactone blocks the hormones that cause follicle miniaturization.
Studies show that combination therapy produces better results than either treatment alone. In one study, 94.1% of men using both minoxidil and finasteride showed improvement, compared to 80.5% using minoxidil alone and 59% using finasteride alone. The treatments have synergistic effects.
Microneedling is another powerful addition. Using a derma roller or derma pen to create controlled micro-injuries in the scalp enhances minoxidil absorption and triggers the release of growth factors. Research shows that microneedling plus minoxidil produces significantly better results than minoxidil alone, in some studies, nearly double the hair count improvement. The protocol: microneedle once a week (1.0-1.5mm depth), wait 24 hours, then resume minoxidil.
Low-level laser therapy (LLLT) is FDA-cleared for hair loss and can be used alongside minoxidil. Devices like laser caps or combs use red light wavelengths to stimulate cellular activity in follicles. The evidence is mixed, but some studies show modest improvement in hair density when combined with topical treatments.
What about natural supplements? Certain ingredients like saw palmetto, biotin, and marine collagen may support hair health, but the evidence is weaker than for pharmaceutical treatments. If you’re going to add supplements, do so in addition to minoxidil, not instead of it. And be aware that many hair supplement claims are not backed by rigorous science.
One critical rule: if you’re combining treatments, introduce them one at a time. Start with minoxidil for at least 3 months, assess your response, then add a second treatment if needed. This allows you to identify what’s working and what’s causing side effects.
What Happens If You Stop Using Minoxidil?
This is the part nobody wants to hear: minoxidil is not a cure. It’s a treatment. If you stop using it, you’ll lose the hair you gained within 3-6 months. The follicles will return to their pre-treatment state, and the underlying pattern hair loss will continue.
Why? Because minoxidil doesn’t address the root cause of androgenetic alopecia, which is genetic sensitivity to dihydrotestosterone (DHT). It stimulates growth and prolongs the anagen phase, but it doesn’t stop the hormonal process that’s causing follicles to shrink. When you remove the stimulus (minoxidil), the follicles revert.
This is why minoxidil is considered a lifelong commitment. You’re not using it for a year to “fix” your hair, you’re using it indefinitely to maintain the improvement. For some people, this is a dealbreaker. For others, it’s an acceptable trade-off for visible results.
There is one exception: if your hair loss was temporary (telogen effluvium from stress, illness, or nutritional deficiency), minoxidil can help speed recovery, and you may be able to stop once the underlying cause is resolved and your hair has returned to baseline. But if you have genetic pattern hair loss, stopping minoxidil means losing your gains.
Some people try to taper off gradually, reducing from twice daily to once daily, then to every other day. This doesn’t work. You’ll just lose results more slowly. If you’re going to use minoxidil, commit to the protocol. If you’re not willing to use it long-term, consider whether it’s worth starting.
Troubleshooting: When Minoxidil Isn’t Working
You’ve been using minoxidil consistently for six months. You’ve pushed through the shedding phase. But when you look in the mirror, you’re still not seeing the results you expected. What now?
First, verify that you’re actually a non-responder and not just experiencing slower-than-average results. Take photos in consistent lighting (same time of day, same angle) and compare month 0 to month 6. Look for subtle changes: finer hairs along the hairline, increased density in thinning areas, thicker individual strands. Sometimes the improvement is gradual enough that you don’t notice it day-to-day, but it’s visible in photos.
If there’s genuinely no improvement, consider these factors. Are you applying minoxidil to a clean, dry scalp? Are you leaving it on for at least 4 hours before washing? Are you using the full 1ml dose twice daily? These seem like basic questions, but inconsistent application is the most common reason for poor results.
Check your scalp condition. If you have significant buildup from hard water, sebum, or styling products, minoxidil can’t penetrate effectively. This is where a chelating shampoo becomes essential. If you haven’t been using one, start now and give it another 3 months. Many “non-responders” in the Gulf region are actually dealing with absorption issues, not true treatment resistance.
Consider whether you’re a sulfotransferase deficient non-responder. Minoxidil is a prodrug, it needs to be converted to minoxidil sulfate by an enzyme called sulfotransferase to become active. About 10-20% of people have low levels of this enzyme, which means they don’t respond well to topical minoxidil. If this is the case, you might respond better to oral minoxidil (which bypasses the need for scalp conversion), but that requires a prescription and medical supervision.
Finally, reassess your diagnosis. If minoxidil isn’t working at all, it’s possible you don’t have androgenetic alopecia. Conditions like alopecia areata, scarring alopecia, or hair loss due to thyroid disease won’t respond to minoxidil. See a dermatologist or trichologist for a proper diagnosis, possibly including a scalp biopsy or blood work.
References
- A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men - PubMed
- Hair Loss: Diagnosis and Treatment - American Academy of Dermatology
- Hardness of Water - US Geological Survey
- Treatment of female pattern hair loss with oral antiandrogens - PubMed
- Microneedling as an adjuvant therapy for androgenetic alopecia - PubMed