You’ve noticed your hairline creeping backward. Not in the typical male pattern baldness way, this is different. It’s a band of smooth skin where hair used to grow, and it’s moving steadily up your forehead. Your eyebrows are thinning too, especially at the outer edges. You’re not imagining it.
This is frontal fibrosing alopecia (FFA), a scarring form of hair loss that’s become increasingly common among women over 50. Twenty years ago, most dermatologists had never seen a case. Today, it accounts for a significant percentage of hair loss consultations in post-menopausal women across the Gulf region and worldwide.
Here’s what makes FFA particularly challenging: it’s permanent. The hair follicles aren’t dormant, they’re destroyed and replaced with scar tissue. But caught early and treated aggressively, progression can be stopped. That’s why understanding the signs matters.
This article contains affiliate links. See our affiliate disclosure for details.
What Frontal Fibrosing Alopecia Actually Is
Frontal fibrosing alopecia is a subtype of lichen planopilaris, a scarring (cicatricial) alopecia that destroys hair follicles through chronic inflammation. The defining characteristic is a band-like recession of the frontal hairline, typically symmetrical, moving backward from the temples and forehead.
Unlike androgenetic alopecia (common pattern hair loss), FFA doesn’t thin the hair. It eliminates it completely. The affected skin becomes smooth, sometimes slightly pale or shiny, with visible loss of the tiny vellus hairs (peach fuzz) that normally cover the hairline area.
The condition was first described in 1994 by Dr. Steven Kossard in Australia. Since then, incidence has surged globally. A 2017 study in the British Journal of Dermatology documented a 10-fold increase in FFA cases between 2004 and 2016 in the UK alone.
FFA primarily affects post-menopausal women, with average onset around age 60. But it’s increasingly diagnosed in younger women (40s) and occasionally in men. The Gulf region has seen rising case numbers, though whether this reflects true increased incidence or improved diagnostic awareness remains debated.
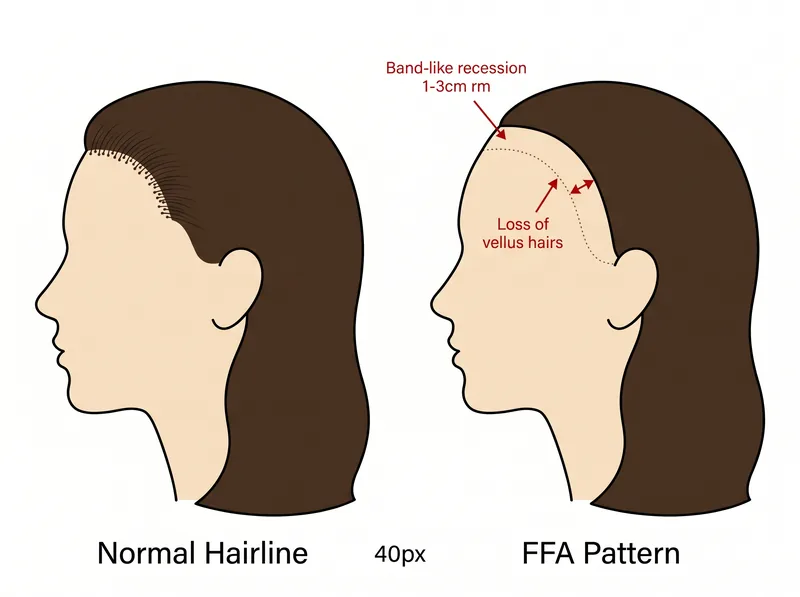 The characteristic band-like pattern of frontal fibrosing alopecia compared to a normal hairline, showing the gradual recession and loss of the frontal hairline.
The characteristic band-like pattern of frontal fibrosing alopecia compared to a normal hairline, showing the gradual recession and loss of the frontal hairline.
The Warning Signs You Shouldn’t Ignore
Early detection is critical because FFA is progressive. Once follicles are destroyed, they can’t regenerate. The earlier you catch it, the more hair you can save.
The most common early sign isn’t actually hairline recession, it’s eyebrow loss. Many women notice their eyebrows thinning, particularly at the lateral (outer) third, months or even years before the frontal hairline starts receding. This can be subtle at first, dismissed as normal aging or over-plucking.
Hairline recession in FFA follows a characteristic pattern. It’s not patchy or random. You’ll see a band of hairless skin, usually 1-3 centimeters wide, that moves backward symmetrically from your original hairline. The skin in this band is smooth, often slightly lighter than surrounding skin, and completely lacks vellus hairs.
Other warning signs include loss of sideburn hair, thinning or complete loss of body hair (arms, legs, pubic area), and facial papules (small bumps) along the hairline. Some women report itching, burning, or tenderness along the affected hairline, though many have no symptoms at all.
If you’re experiencing progressive hairline recession combined with eyebrow thinning, don’t wait. See a dermatologist immediately. Early intervention is the only way to prevent extensive permanent loss.
 Eyebrow loss is one of the earliest and most common signs of FFA, often appearing before noticeable hairline recession.
Eyebrow loss is one of the earliest and most common signs of FFA, often appearing before noticeable hairline recession.
Why FFA Happens: The Frustrating Truth
Here’s the honest answer: we don’t fully know what causes frontal fibrosing alopecia. The rapid increase in cases over the past two decades suggests an environmental trigger, but identifying it has proven extraordinarily difficult.
The leading hypothesis involves an autoimmune component. In FFA, the immune system appears to attack hair follicles, specifically targeting the follicular stem cell niche. This triggers chronic inflammation that ultimately destroys the follicle and replaces it with scar tissue. But what initiates this immune attack remains unclear.
Hormonal factors play a role. The condition predominantly affects post-menopausal women, suggesting estrogen decline may be involved. However, hormone replacement therapy hasn’t shown consistent protective effects, and the condition also occurs in pre-menopausal women and men, complicating the hormonal theory.
Environmental and lifestyle factors are under intense investigation. Research published in the Journal of the European Academy of Dermatology and Venereology found associations between FFA and use of facial sunscreens, certain cosmetic products, and specific hair care practices. However, these associations don’t prove causation, and the findings remain controversial.
Genetic susceptibility likely matters. FFA shows familial clustering, and certain HLA (human leukocyte antigen) types appear more common in affected individuals. But no single gene has been identified as causative.
The Gulf region’s unique environmental factors, intense UV exposure, high mineral content in water, widespread use of hair straightening treatments, have led researchers to investigate whether these contribute to the rising incidence locally. Hard water, in particular, can damage the scalp barrier. While mineral buildup alone doesn’t cause FFA, maintaining scalp health with a chelating shampoo like Regrowth+ may help reduce scalp inflammation that could potentially exacerbate underlying autoimmune processes.
Getting an Accurate Diagnosis
FFA diagnosis requires clinical expertise. It’s not something you can self-diagnose from photos online, and it’s often missed or misdiagnosed by non-specialist physicians.
A dermatologist experienced in hair disorders will start with a thorough clinical examination. They’ll assess your hairline pattern, check for eyebrow loss, examine your scalp for signs of inflammation or scarring, and look for loss of vellus hairs, a hallmark of FFA that distinguishes it from traction alopecia or other causes of hairline recession.
Dermoscopy (trichoscopy) is essential. This magnified examination reveals characteristic features: perifollicular erythema (redness around follicles), perifollicular scale, loss of follicular openings in affected areas, and the absence of vellus hairs. These findings help confirm FFA and rule out other conditions.
In many cases, a scalp biopsy is necessary for definitive diagnosis. The biopsy will show lymphocytic inflammation around hair follicles, follicular destruction, and replacement with fibrous tissue, the pathological hallmarks of scarring alopecia. The biopsy also helps rule out other scarring alopecias that may look similar clinically.
Blood work is typically ordered to exclude other conditions that can cause hair loss: thyroid dysfunction, iron deficiency, autoimmune diseases like lupus. While these tests won’t diagnose FFA, they’re important for ruling out treatable causes of hair loss that may coexist.
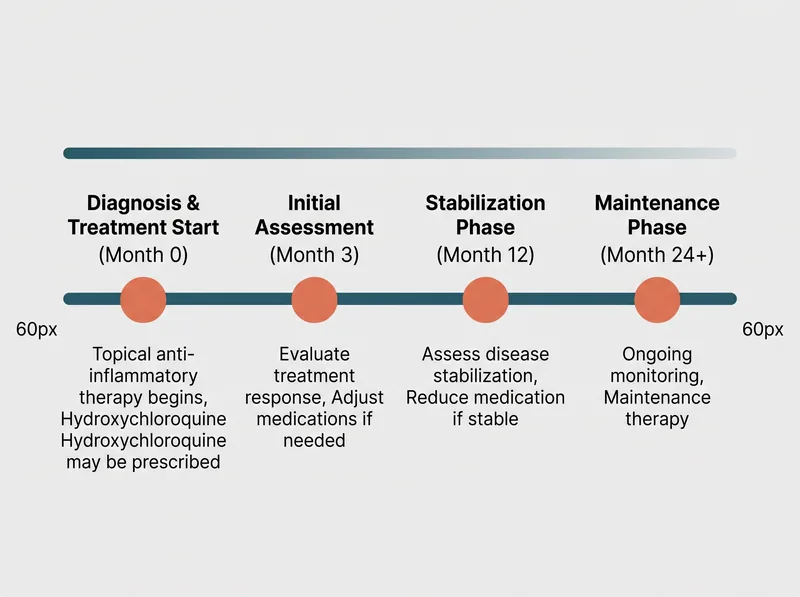 FFA treatment requires long-term commitment, with most patients needing 12-24 months to see stabilization and ongoing maintenance to prevent progression.
FFA treatment requires long-term commitment, with most patients needing 12-24 months to see stabilization and ongoing maintenance to prevent progression.
Treatment Options That Actually Work
Let’s be clear: there’s no cure for frontal fibrosing alopecia. Treatment goals are to stop progression, reduce inflammation, and preserve remaining hair. Lost hair won’t grow back, but you can prevent further loss if treatment starts early.
First-line treatment typically involves topical corticosteroids. High-potency topical steroids (like clobetasol propionate) applied to the affected hairline can reduce inflammation. They’re usually prescribed for intermittent use (a few weeks on, a few weeks off) to minimize side effects like skin atrophy.
Intralesional corticosteroid injections are another option. A dermatologist injects diluted triamcinolone acetonide directly into the affected hairline every 4-8 weeks. This delivers anti-inflammatory medication directly to the follicles. It’s more effective than topical application but requires in-office visits.
Hydroxychloroquine, an antimalarial medication with immunomodulatory properties, has become a cornerstone of FFA treatment. A 2019 study in the Journal of the American Academy of Dermatology showed that hydroxychloroquine stabilized disease progression in approximately 60% of FFA patients. It’s typically prescribed at 200-400mg daily, requires regular eye exams to monitor for rare retinal toxicity, and takes 3-6 months to show effect.
5-alpha reductase inhibitors, finasteride (1-2.5mg daily) or dutasteride (0.5mg daily), are sometimes used, particularly in men with FFA or women who can’t take hydroxychloroquine. These medications block DHT (dihydrotestosterone), though the exact mechanism of benefit in FFA isn’t fully understood since FFA isn’t primarily androgen-driven.
Combination therapy is common. Many dermatologists prescribe hydroxychloroquine as a systemic treatment plus topical or intralesional steroids for localized inflammation. The goal is to attack the inflammatory process from multiple angles.
What doesn’t work: minoxidil. While minoxidil is effective for androgenetic alopecia, it doesn’t address the scarring inflammation in FFA. Once follicles are destroyed, no growth stimulant can revive them.
Lifestyle Modifications and Scalp Care
Beyond medical treatment, certain lifestyle modifications may help slow progression, though evidence is mostly observational rather than from controlled trials.
Minimize scalp trauma. Avoid tight hairstyles, harsh chemical treatments, and aggressive brushing along the hairline. While traction didn’t cause your FFA, mechanical stress on already-inflamed follicles can worsen damage.
Sunscreen use on the scalp and hairline is recommended. UV exposure may trigger inflammation in susceptible individuals. Use a mineral-based sunscreen (zinc oxide or titanium dioxide) rather than chemical filters, as some research has suggested possible associations between certain chemical sunscreens and FFA, though this remains unproven.
Gentle, pH-balanced hair care is important. The scalp barrier is already compromised by inflammation. Harsh sulfates, high-alkaline shampoos, and mineral buildup from hard water can add insult to injury. Hard water is particularly problematic in the Gulf region, depositing calcium and magnesium that can irritate sensitive scalps.
Some dermatologists recommend avoiding leave-on facial cosmetics along the hairline, based on observational data suggesting possible associations. The evidence isn’t strong enough to make this a universal recommendation, but if you’re using heavy creams or makeup near your hairline, discuss with your dermatologist whether temporarily discontinuing might be worth trying.
Diet and supplements haven’t shown benefit specific to FFA. Unlike iron deficiency or nutritional alopecia, FFA isn’t driven by nutritional factors. That said, overall health improvation, managing stress, eating a balanced diet, addressing any coexisting deficiencies, supports your body’s ability to respond to treatment.
What to Expect: Prognosis and Long-Term Management
FFA is a chronic condition. Even with treatment, it requires long-term management and monitoring. Understanding realistic expectations is crucial.
Treatment success is measured by stabilization, not regrowth. If your hairline stops receding and inflammation subsides, treatment is working. Lost hair won’t return, but you’ve preserved what remains. This is why early intervention is so critical, there’s more to save.
Response to treatment varies. Some women achieve complete stabilization within 6-12 months. Others experience slower progression despite treatment, requiring medication adjustments or combination approaches. Approximately 30-40% of patients show ongoing progression even with aggressive therapy, though usually at a slower rate than without treatment.
Eyebrow loss often continues even when hairline progression stabilizes. This is frustrating but common. Eyebrow transplantation is an option once the disease is stable, though transplanted hairs can be affected by ongoing inflammation if disease activity persists.
Monitoring is lifelong. Even if your FFA stabilizes and you discontinue or reduce medications, regular dermatology follow-ups are necessary. Reactivation can occur, and early detection of renewed progression allows for prompt treatment adjustment.
The psychological impact shouldn’t be underestimated. Progressive, permanent hair loss affects self-image and confidence. Many women with FFA experience anxiety, depression, and social withdrawal. Connecting with support groups, working with a therapist familiar with chronic skin conditions, and exploring cosmetic solutions (wigs, hairline makeup, microblading for eyebrows) can help.
Realistic timelines matter. You won’t see improvement in weeks. It takes 3-6 months to assess whether a treatment is working, and 12-24 months to achieve optimal stabilization. Patience and consistency with treatment are essential.
Surgical Options: When and Whether to Consider Them
Hair transplantation for FFA is controversial and requires careful patient selection. Unlike androgenetic alopecia where transplants are highly successful, FFA presents unique challenges.
The fundamental problem: FFA is an active inflammatory process. Transplanting hair into inflamed tissue carries high risk of graft failure and can potentially trigger disease flare in the transplanted area. Most hair transplant surgeons won’t operate on active FFA.
Timing is critical. Transplantation should only be considered after disease has been stable (no progression) for at least 1-2 years with ongoing treatment. Even then, success rates are lower than for non-scarring alopecia, and there’s risk of losing transplanted grafts to ongoing inflammation.
Eyebrow transplantation has higher success rates than hairline restoration in FFA patients, possibly because eyebrow follicles are less susceptible to the inflammatory process. Many women opt for eyebrow transplants once disease is stable, accepting that hairline restoration is too risky.
Alternative cosmetic solutions often make more sense. Hairline tattooing (scalp micropigmentation) can create the illusion of a fuller hairline without the risks of surgery. High-quality wigs or hairpieces designed for frontal hairline coverage provide immediate cosmetic improvement without medical risk. Microblading for eyebrows is widely available and effective.
If you’re considering surgical intervention, consult with a hair transplant surgeon who has specific experience with scarring alopecia. They should work closely with your dermatologist to assess disease stability and surgical candidacy. Don’t rush this decision.
References
- Frontal fibrosing alopecia: A retrospective review of 62 patients from 2 centers - British Journal of Dermatology
- Frontal fibrosing alopecia: A retrospective study of 120 patients - Journal of the European Academy of Dermatology and Venereology
- Treatment of frontal fibrosing alopecia: A systematic review - Journal of the American Academy of Dermatology
- Frontal Fibrosing Alopecia - American Academy of Dermatology
- Cicatricial Alopecia Research Foundation - FFA Information - CARF